Recherche
Recherche en cours
Trauma NB a non seulement le mandat d’accroître la capacité de recherche, mais il participe aussi activement à la recherche. Voici quelques projets que Trauma NB a actuellement en cours :
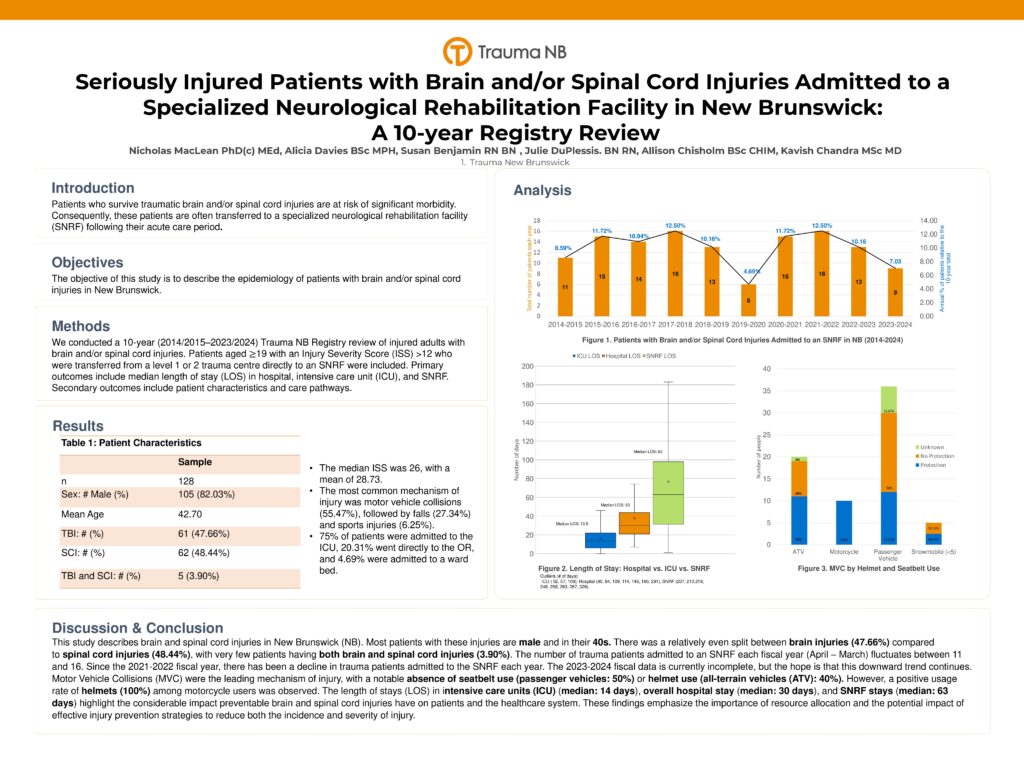
Chutes et patients gravement blessés au Nouveau-Brunswick : une revue du registre sur neuf ans
Accidents de véhicules à moteur et patients gravement blessés au Nouveau-Brunswick
Analgésie et sédation après l’intubation au service d’urgence pour les patients blessés : présentation d’une intervention éducative
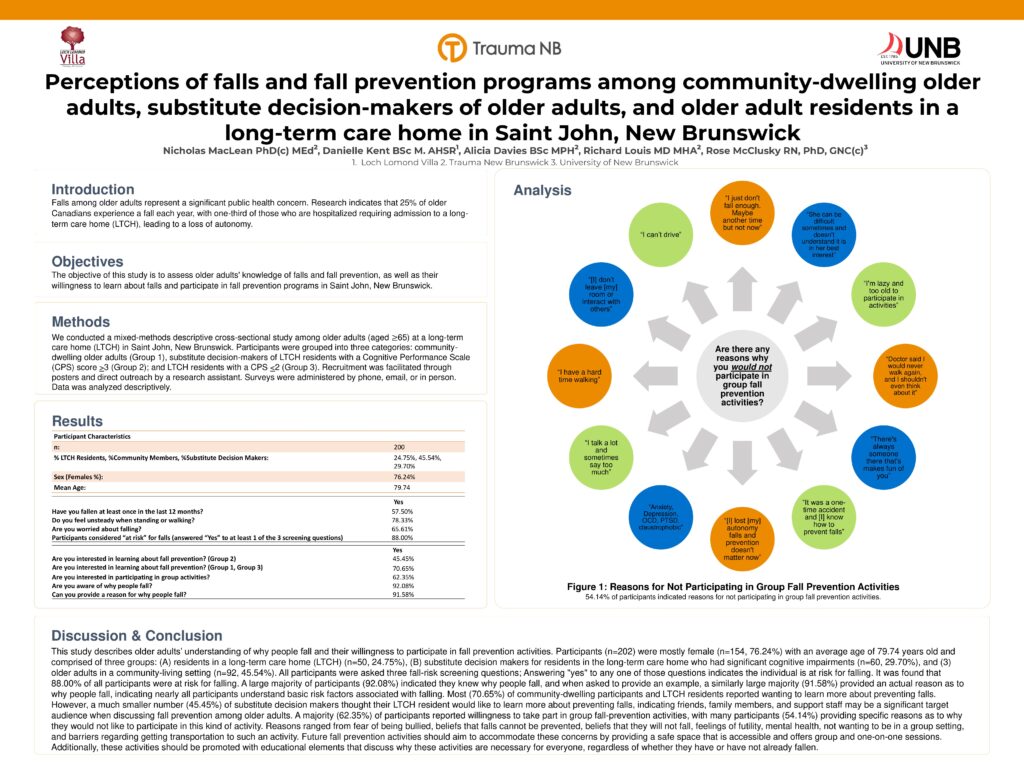
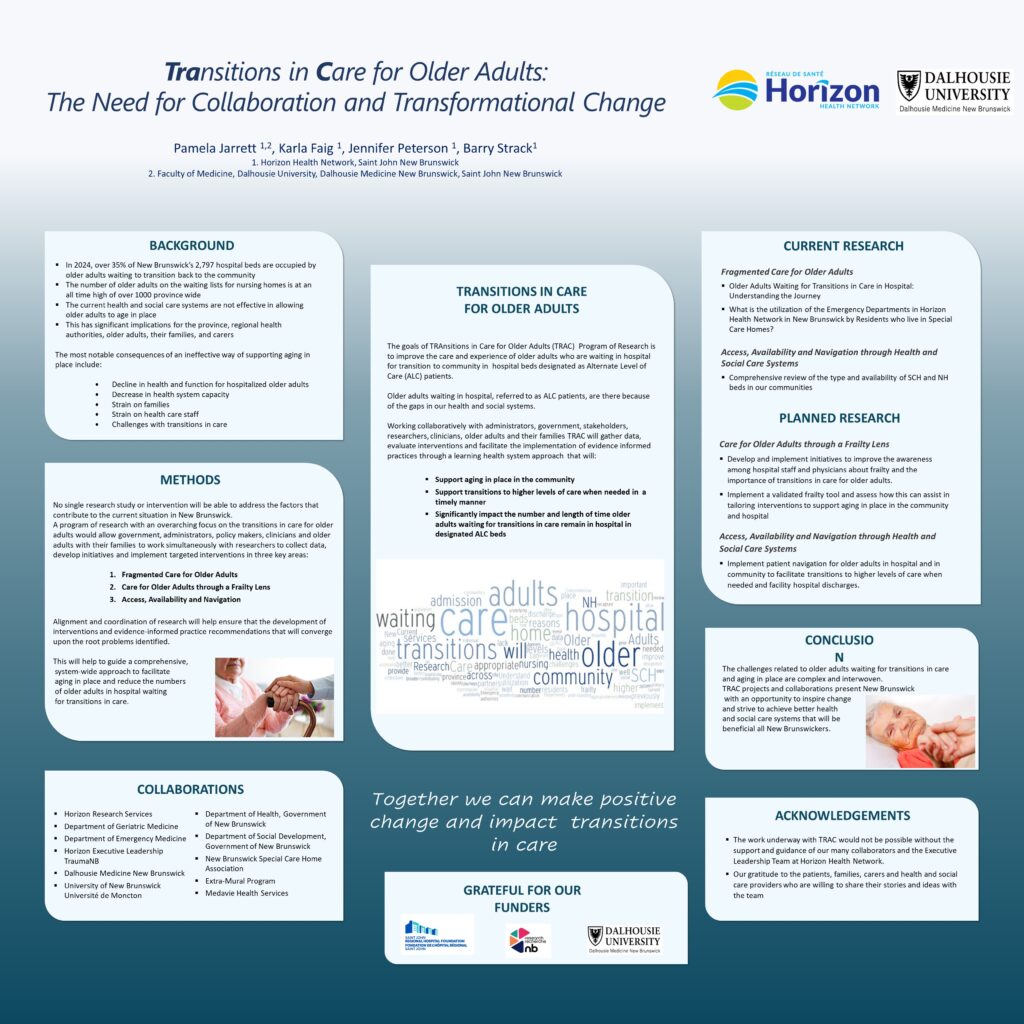
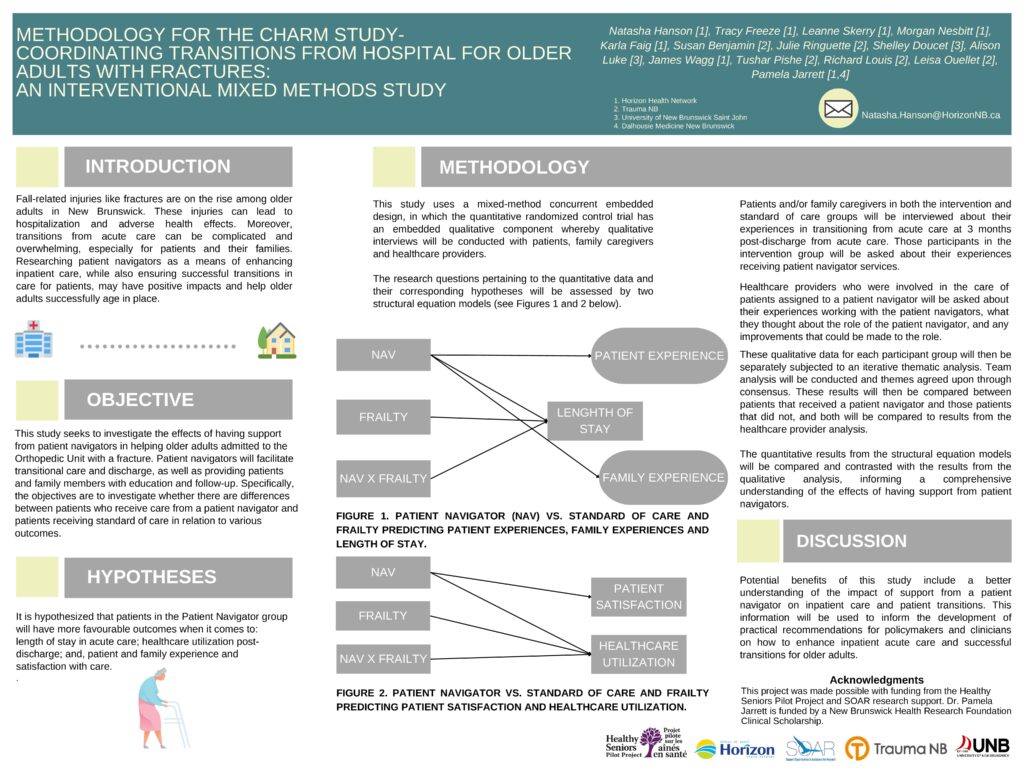
Soutenir les personnes âgées lors des transitions dans la prestation de soins : comment les intervenants pivots peuvent aider les patients
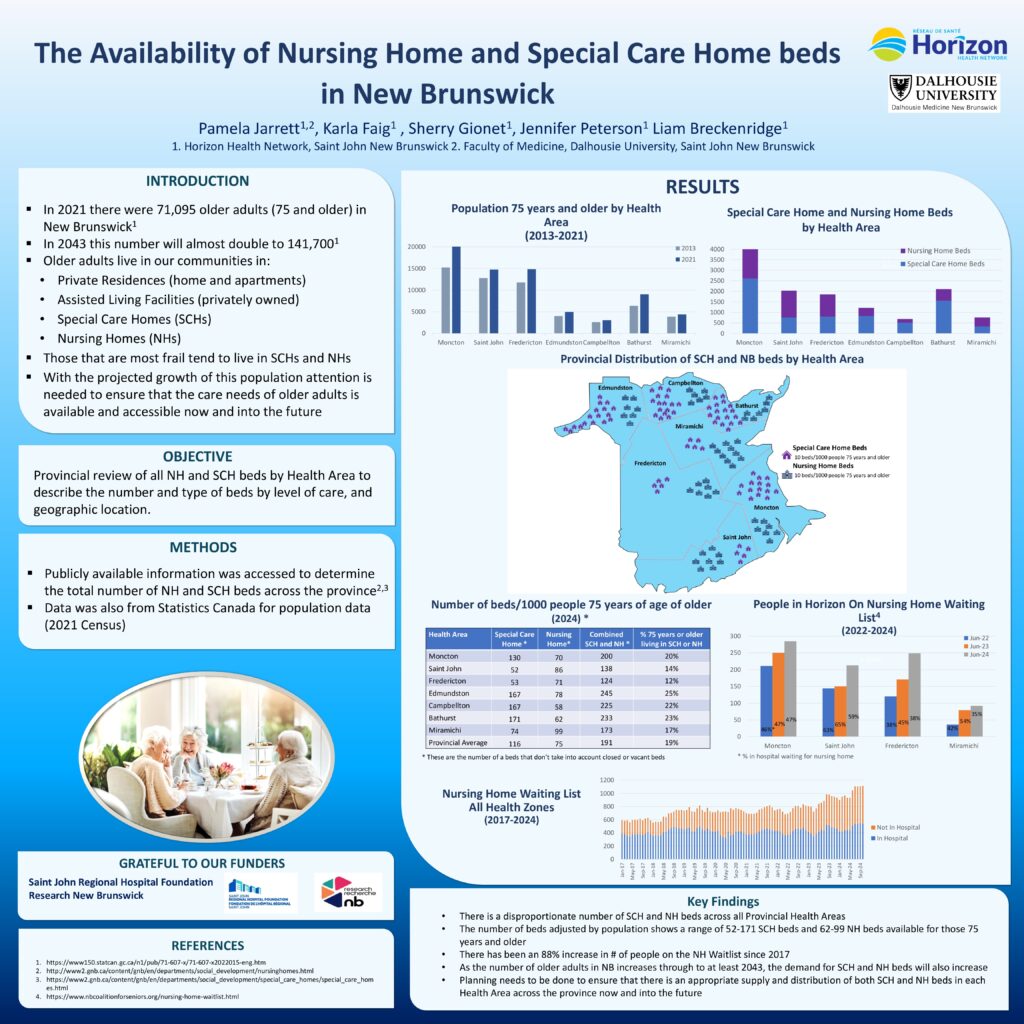
Les personnes âgées en attente d’une transition dans la prestation de soins à l’hôpital : comprendre le parcours
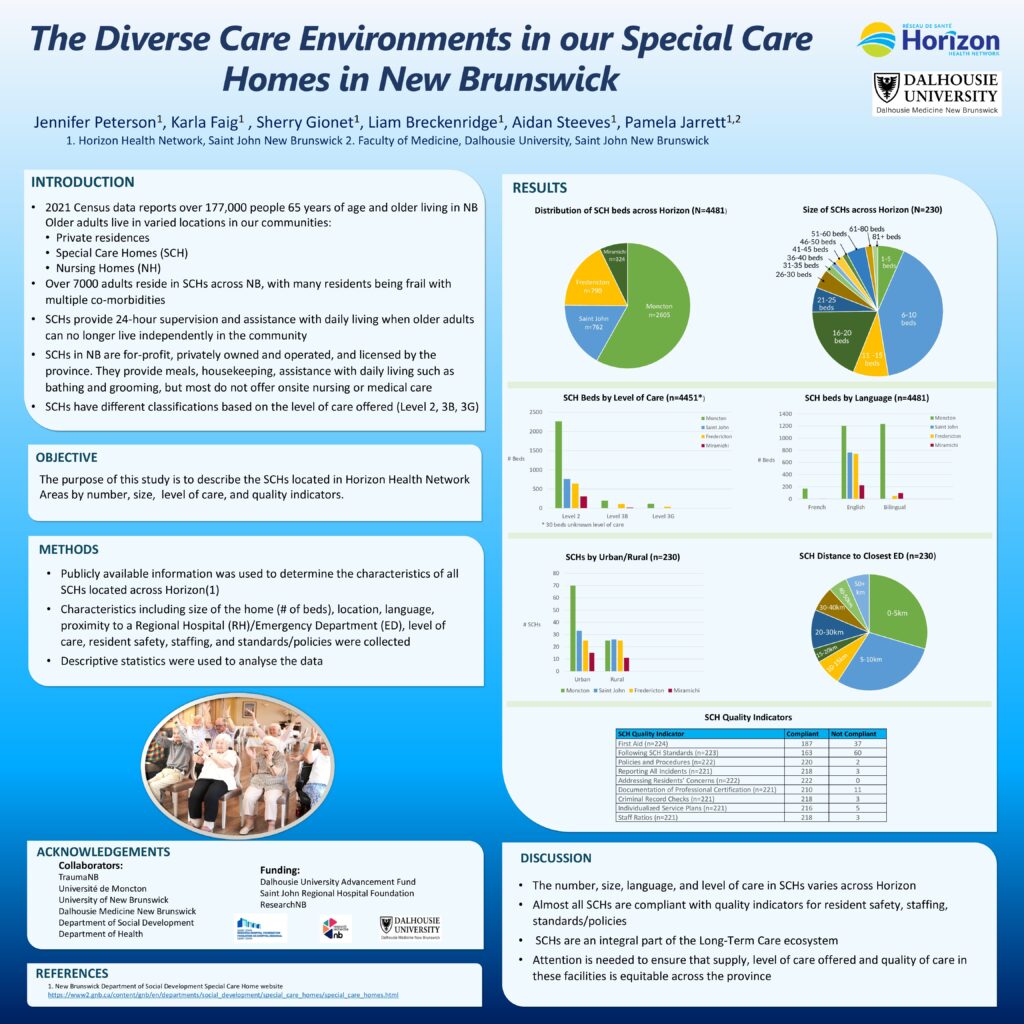
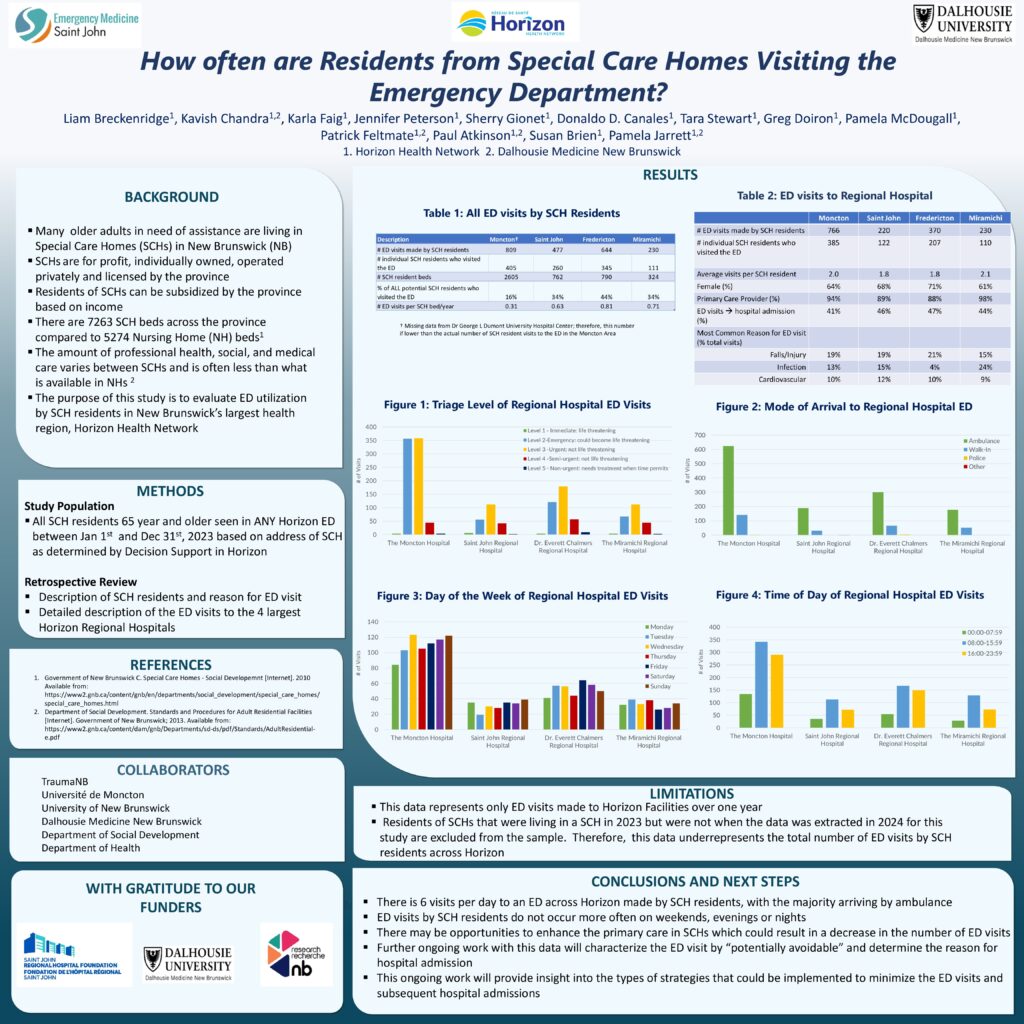
Quelle est l’utilisation des services d’urgence du Réseau de santé Horizon au Nouveau-Brunswick par les résidents des foyers de soins spéciaux

Soutien aux chercheurs
Trauma NB investit dans l’accroissement de la capacité de recherche sur les traumatismes au Nouveau-Brunswick. Le Sous-comité de recherche de Trauma NB assure une surveillance stratégique de la recherche au sein du programme, en mettant plus particulièrement l’accent sur l’épidémiologie descriptive des traumatismes au Nouveau-Brunswick. Pour en savoir plus, veuillez prendre contact avec allison.chisholm@horizonnb.ca
Soutien externe à la recherche :
Pour ce qui est des politiques de recherche, nous avons adopté les mêmes que les réseaux de santé Horizon et Vitalité. Pour obtenir de plus amples renseignements, cliquez sur les liens suivants ou communiquez directement avec les services de recherche de Vitalité à recherche.research@vitalitenb.ca ou avec les services de recherche d’Horizon à researchservices@horizonnb.ca

Dr. Kavish Chandra
MD MSc CCFP(EM)
Président, Sous-comité de recherche
Kavish Chandra MD MSc CCFP(EM)
Président, Sous-comité de recherche de Trauma NB
Après avoir passé son enfance dans le nord-ouest de la Colombie-Britannique, le Dr. Kavish Chandra s’est installé au Nouveau-Brunswick pour poursuivre ses études de premier cycle et de deuxième cycle à l’Université Mount Allison. Il a ensuite suivi le programme de formation médicale Dalhousie Medicine New Brunswick et a effectué sa résidence en médecine d’urgence et en médecine familiale à l’Université Dalhousie.
Le Dr. Chandra exerce actuellement la médecine en tant qu’urgentologue et s’intéresse particulièrement à la gestion des voies respiratoires, à la traumatologie et à la réanimation, à la formation médicale, à la recherche et à l’échographie au point d’intervention.
Nomination
- Urgentologue, Service de médecine d’urgence, Réseau de santé Horizon, région de Saint John
- Professeur adjoint d’enseignement clinique, Département de médecine d’urgence, Université Dalhousie
- Directeur de la recherche, Service de médecine d’urgence, Hôpital régional de Saint John
- Chef provincial du Réseau d’intervention rapide pour les services d’urgence COVID-19 (CEDRRN) pour le Nouveau-Brunswick
- Chef provincial du Consortium canadien de recherche en réanimation (CanROC) pour le Nouveau-Brunswick
La capacité de recherche au Nouveau-Brunswick est en croissance, et un certain nombre de groupes font la promotion de la recherche locale. Vous trouverez ci-dessous des groupes externes axés sur la recherche au Nouveau-Brunswick.
Recherche publiée
Cliquez sur les travaux ci-dessous pour accéder à la recherche publiée par les membres de Trauma NB.
Les recherches sont publiées exclusivement en anglais. Trauma NB peut posséder une version française de certaines études, qui sont sujettes à disponibilité. Si vous désirez recevoir une copie française, veuillez communiquer avec TraumaNB@HorizonNB.ca
2025 Affiche de la conférence TAC

2024 Affiche de la conférence TAC

2024 Affiche du symposium sur la recherche en santé au Nouveau-Brunswick

2019 Affiche de la conférence TAC
Priest L, Flewelling A, Atkinson P, et al. (March 13, 2025)A Multi-year Review of Major Off-Road Vehicle Injuries and Deaths in New Brunswick.
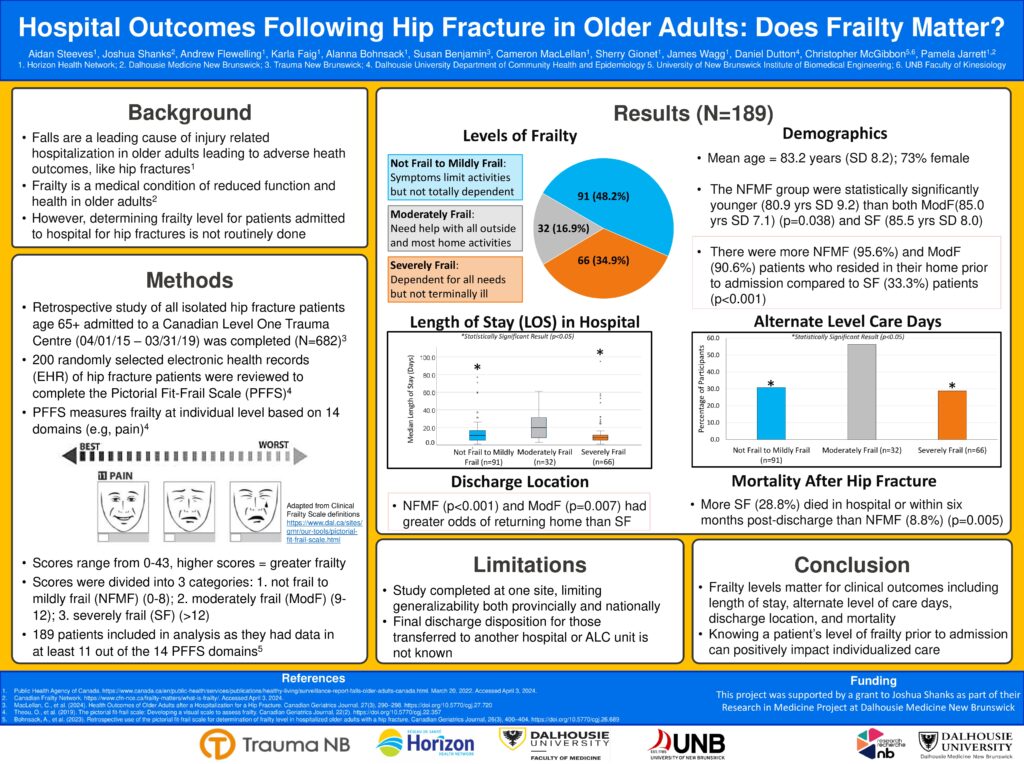
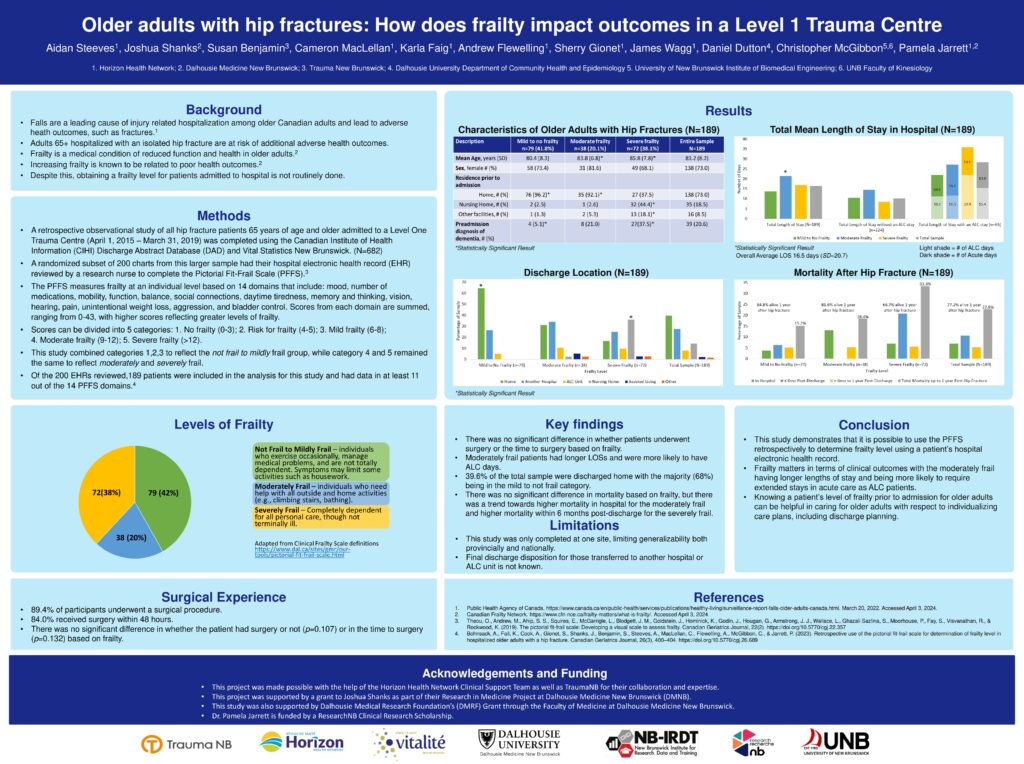
MacLellan, C., Faig, K., Cooper, L., Benjamin, S. ., Shanks, J. ., Flewelling, A. J., Dutton, D. J., McGibbon, C., Bohnsack, A., Wagg, J., & Jarrett, P. (2024). Health Outcomes of Older Adults after a Hospitalization for a Hip Fracture
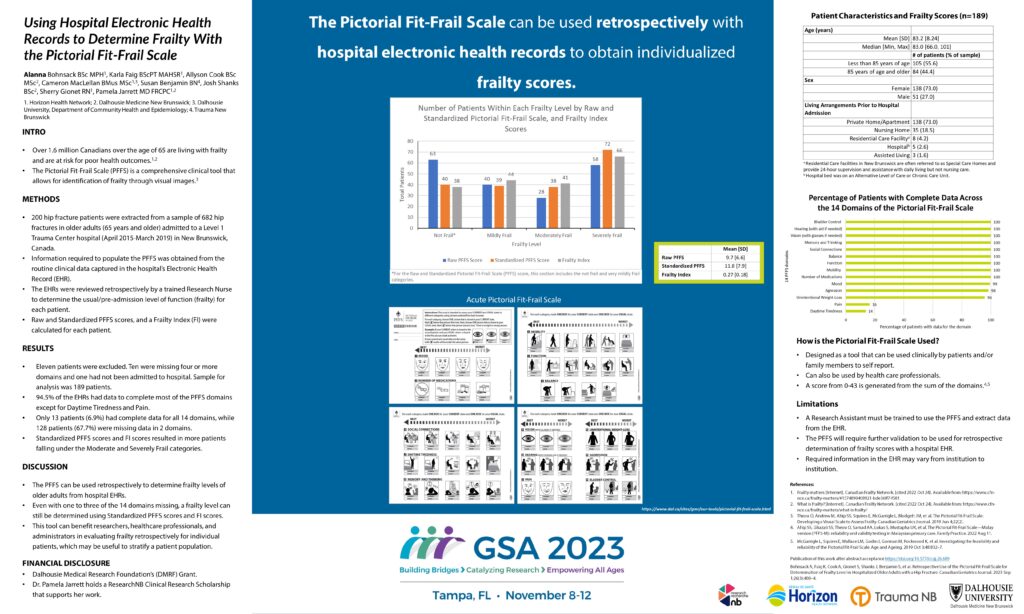
Bohnsack, A., Faig, K. ., Cook, A., Gionet, S., Shanks, J., Benjamin, S., Steeves, A. ., MacLellan, C., Flewelling, A. ., McGibbon, C., & Jarrett, P. (2023). Retrospective Use of the Pictorial Fit-Frail Scale for Determination of Frailty Level in Hospitalized Older Adults with a Hip Fracture.
Chisholm A., Ouelett L., Pishe T., Ringuette J., Watson I. (2021). Are early specialist consultations helpful predictors of those who require care in level 1 or 2 designated trauma centres? TAC. (Résumé de recherche oral primé)
Benjamin S., McEachern S., Watson I. (2021). Was the introduction of a provincially standardized consensus statement for postintubation analgesia and sedation associated with increased use of associated pharmacological therapies in New Brunswick? TAC. (Résumé sur affiche primé)
Benjamin S., Watson I. (2021). Are there important variations in the care of adult trauma patients with isolated, nonoperative subdural hematomas between those admitted to a neurosurgical centre and those admitted to a non-neurosurgical centre for their entire inpatient stay? TAC.
Benjamin S., Chisholm A., Ouelett L., Totton L., Vautour J., Watson I. (2021). Is the use of business intelligence software helpful in planning injury prevention campaigns? TAC.
McEachern S., Ringuette J., Watson I. (2021). Exposure to endotracheal intubation among trauma patients in level 5 trauma centres in New Brunswick — a retrospective review. TAC.
Hickling, A., Mallory, K.D., Wilson, K.E. et al. (2020). The youth concussion awareness network (You-CAN) – a school-based peer-led intervention to improve concussion reporting and social support: the protocol for a cluster randomized trial. BMC Public Health 20, 186.
Benjamin S., Chisholm A., Watson I. (2019). Field trauma triage in New Brunswick: Understanding the « Immediate Life Threat » population TAC
Benjamin, S, Chisholm, A, Watson, I (2019). What are the characteristics of field trauma triage « Bypass Failures » in an integrated, inclusive provincial trauma system? TAC
Hanlon R., French J., Atkinson P., Fraser J., Benjamin S., Poon (2019). Designing team success – an engineering solution to avoid chest tube equipment chaos using best available evidence, consensus and prototyping. Abstract Journal Canadian Journal of Emergency Medicine; 21(S1):S52
Hanlon R, French J, Atkinson P, Fraser J, Benjamin S, Poon (2019). Designing team success – an engineering approach to capture team procedural steps to develop microskills for interprofessional skills education: Abstract Journal Canadian Journal of Emergency Medicine; 21(S1):S85-86
French J., Maclean D., Fraser J., Benjamin S., Atkinson P. (2018). P050: How aware is safe enough? Situational awareness is higher in safer teams doing simulated emergency airway cases. Can J Emerg Med, 20(S1), S74-S74.
French J., Maclean D., David K., McCoy A., Benjamin S., Fraser J., Pishe T., Atkinson P.(2018). P049: Changes in situational awareness of emergency teams in simulated trauma cases using an RSI checklist. Can J Emerg Med, 20(S1), S74-S74.
French J., David K., Benjamin S., Fraser J., Mekwan J., Atkinson P. (2018)MP19: Interprofessional airway microskill checklists facilitate the deliberate practice of direct intubation with a bougie and airway manikins. Can J Emerg Med, 20(S1), S47-S47.
French J., David K., Benjamin S., Fraser J., Mekwan J., Atkinson P. (2018). Interprofessional airway microskill checklists facilitate the deliberate practice of surgical cricothyrotomy with 3-D printed surgical airway trainers. Can J Emerg Med, 20(S1), S73-S74.
Hayre J., Rouse C., French J., Fraser J., Watson I., Benjamin S., Chisholm A., Stoica G., Sealy B., Erdogan M., Green R., Atkinson P. (2018) A traumatic tale of two cities: A comparison of outcomes for adults with major trauma who present to differing trauma centres in neighbouring Canadian provinces. Can J Em Med 20(2); 191-199.
Watson I., Benjamin S., Chisholm A., Ellis K., Pishe T. (2018) Rollover motor vehicle crashes in New Brunswick: A descriptive study. Can J Surg 61 (2 Supp 1) S9.
Watson I., Ellis K., Chisholm A., Pishe T. (2018) Does the presence of CT scanning in level V centres delay access to defintive care? A retrospective review from New Brunswick’s inclusive trauma system. Can J Surg 61 (2 Supp 1) S9.
Benjamin S., Watson I., Chisholm A., Pishe T. (2018) An evaluation of overtriage in New Brunswick’s field trauma triage system. Can J Surg 61 (2 Supp 1) S9.
Benjamin S., Watson I., Chisholm A., Pishe T. (2018) Major trauma and field trauma triage in New Brunswick. Can J Surg 61 (2 Supp 1) S10.
Benjamin S., Atkinson P., Fraser J., French J. (2018) How aware is safe enough? Situational awareness is higher in safer teams doing simulated emergency airway cases CJEM; 20(Supp1):S74
Robinson B., Ellis K., Holland M., Chisholm A., Watson I. (2018) Building a model for assessing trauma-related mortality in a rural trauma system. Can J Surg 61 (2 Supp 1) S10.
Rouse C., Hayre J., French J., Fraser J., Watson I., Benjamin S., Chisholm A., Sealy B., Erdogan M., Green R.S., Stoica G., Atkinson P. (2018) A traumatic tale of two cities: does EMS level of care and transportation model affect survival in patients with trauma at level 1 trauma centres in two neighbouring Canadian provinces? » Emerg Med J., 35(2): 83 – 88.
2017
2016/2017 TPRF Award Winner – Dr. Neil Branch, Dr. Pamela Jarrett, Dr. James Wagg, Dr. Tushar Pishe, Ian Watson, Sue Benjamin, Dr. Linda Yetman, Dr. Bryn Robinson, Dr. Dan Crouse, Dr. Chris McGibbon & Allison Chisholm for the study: Outcomes in Older Adults with Isolated Hip Fractures: A Comprehensive Study across Regional Hospitals in New Brunswick
Benjamin S., Chisholm A., Watson I., Pishe T. (2017) Understanding clinical hip fracture variation in New Brunswick. Can J Surg 60 (3 Supp 2) S23.
Louis R., Benjamin S., Chisholm A., Pishe T., Watson I. (2017) Concussion and admission diagnosis among seniors who fall: A descriptive analysis. Can J Surg 60 (3 Supp 2) S32.
2016
2015/2016 TPRF Award Winner – Dr. James French, Jacqueline Fraser & Devon McLean for the study: Does the use of an RSI checklist and equipment silhouette in simulated emergency scenarios improve team performance and operational safety?
McLean D., French J., Fraser J., Benjamin S., Atkinson P. (2016) Does the use of an RSI checklist and equipment silhouette in simulated emergency scenarios improve team performance and operational safety? Can J Surg 59 (3 Supp 1) S18.
Benjamin S., Hogan A., Watson I., French J. (2016) Exposure to major trauma patients and safety-critical procedures. Part 1: Risk and reliability. Can J Surg 59 (3 Supp 1) S18.
Orchard J., Cormier C., Chisholm A., French J., Pishe T., Watson I. (2016) Impact of a pre-alert program for air ambulance response to major trauma patients in a provincial, inclusive trauma program: The New Brunswick experience. Can J Surg 59 (3 Supp 1) S19.
Woodford S., Hogan A., Watson I. (2016) Impact of the repeated offering of the Rural Trauma Team Development Course (RTTDC) on trauma transfer intervals in a provincial, inclusive system. Can J Surg 59 (3 Supp 1) S19.
Kenney M., French J., Fraser J., Phlean of Emer B., Watson I., Benjamin S., Chisholm A., Atkinson A. (2016) Out in the sticks and stones may break your bones, but does rurality surely hurt you? Trauma patient health equality in New Brunswick. Can J Surg 59 (3 Supp 1) S19.
Benjamin S., Hogan A., Chisholm A., Watson I. (2016) The timely use of tranexamic acid in trauma. Can J Surg 59 (3 Supp 1) S20.
2015
2014/2015 TPRF Award Winner – Dr. Grant Hanigan, Dr. Gabriel Cormier, Dr. Mathieu Bélanger & Dr. Alier Marrero for the study: Validation of a novel tool, the RT2, for clinical diagnostic accuracy of falls occurrence in persons with Multiple Sclerosis
Phelan B., Fraser J., Pishe T., Middleton J., Chisholm A., Benjamin S., Watson I., Atkinson P. (2015) Severe trauma in the province of New Brunswick: A descriptive epidemiological study. Can J Em Med 17 (Supp1) s77.
Chisholm A., Benjamin S., Hogan A., Woodford S., Watson I. (2015) All in the family: Creating and implementing an inclusive provincial trauma registry. Can J Surg 58 (2 Supp 1) S18.
Hogan A., Woodford S., Watson I. (2015) Lessons learned from a provincial trauma transfer system. Can J Surg 59 (3 Supp 1) S18-S19.
Watson I., Hogan A., Woodford S., Chisholm A., Louis R., St. Pierre E. (2015) Trauma NB : 5 years later. Can J Surg 59 (3 Supp 1) S19.
Hogan A., Louis R. (2015) Provincial coordination of injury prevention: The New Brunswick experience. Can J Surg 59 (3 Supp 1) S19.
Hogan A., Woodford S., Watson I. (2015) Improving access and uptake of Trauma Nursing Core Course (TNCC): A provincial approach. Can J Surg 59 (3 Supp 1) S19.
Hewitson L., Atkinson P., Mekwan J., Verbeul G., Lewis D. (2015) ULTRASIM : Ultrasound in trauma simulation. Does the use of ultrasound during simulated scenarios imrpive diagnostic abilities ? Can J Surg 59 (3 Supp 1) S19-S20.
Rouse C., Hayre J., French J., Watson I., Benjamin S., Fraser J., Chisholm A., Sealy B., Erdogan M., Green R., Atkinson R. (2015) Traumatic tale of 2 cities part I: Does being treated by different EMS affect outcomes in trauma patients destined for transport to level I centres in Halifax and Saint John? Can J Surg 59 (3 Supp 1) S20.
Rouse C., Hayre J., French J., Watson I., Benjamin S., Fraser J., Chisholm A., Sealy B., Erdogan M., Green R., Atkinson R. (2015) Traumatic tale of 2 cities part II: Does being treated by different hospitals affect outcome in trauma patients destined for transport to level I centres in Halifax and Saint John? Can J Surg 59 (3 Supp 1) S20.
Phelan B., Fraser J., Pishe., Middeton J., Chisholm A., Benjamin S., Watson I., Atkinson P. (2015) Severe trauma in the province of New Brunswick: A descriptive epidemiological study. Can J Surg 59 (3 Supp 1) S28.
2014
2013/2014 TPRF Award Winner – Dr. Paul Atkinson & Dr. James French for the study: Tranexamic acid for the treatment of significant traumatic brain injury: an international randomized, double blind placebo controlled trial.
Atkinson, P., French, J., & Nice, C. A. (2014). Procedural sedation and analgesia for adults in the emergency department. BMJ, 348(9), 2965-2977.
Exposure to major trauma management of learners training to become emergency physicians in New Brunswick. Can J Surg 57 (3 Supp 3) S65-S66.
Montazeri R., Wagg J., Mayich J., King H., Swan J., Fraser J., Benjamin S., Atkinson P. (2014) Distal radial fractures: Adequacy of reductions performed in the emergency department. Can J Surg 57 (3 Supp 3) S75.
Boulay R., Richard D., Savoie J-P., Goulette E., Chisholm A., Watson I. (2014) Improving effectiveness of field trauma triage activations in New Brunswick. Can J Surg 57 (3 Supp 3) S75-S76.
Benjamin S., Chisholm A., Watson I. (2014) Field trauma triage guidelines as a predictor of key emergency department time intervals. Can J Surg 57 (3 Supp 3) S76.
2013
2012/2013 TPRF Award Winner – Dr. Leanne Hewitson, Dr. Paul Atkinson, Dr. Glen Verheul & Dr. David Lewis for the study: ULTRASIM: Ultrasound in TRAuma SIMulation. Does ultrasound simulation improve diagnosis during simulated scenarios?
Hogan A. (2013) Sport related concussion care in the emergency department: What every ED nurse needs to know. Can J Em Nursing 36:2; 22-23.
Atkinson P., Fraser J., Benjamin S., Sproul E., Mehta A. (2013) Wake up: Head injury management around the clock. Can J Em Med (15 Supp 1) S22.
Hogan A. (2013) A collaborative approach to reducing injuries in New Brunswick: Acute care and injury prevention. Can J Surg 56 (2 Supp) S27.
Watson I., Boulay R., Chisholm A., Beairsto E., Goulette E., Martin M. (2013) Impact of changes to a provincial field trauma triage tool in New Brunswick. Can J Surg 56 (2 Supp) S28.
Woodford S., Benjamin S., Boulay R., Watson I. (2013) Ensuring quality of field trauma triage in New Brunswick. Can J Surg 56 (2 Supp) S28.
Hogan A., Boulay R., Watson I. (2013) Benefits of a provincial trauma transfer referral system: Beyond the numbers. Can J Surg 56 (2 Supp) S28.
Boulay R., Watson I., Savoie J., Benjamin S., Martin M. (2013) The field trauma triage landscape in New Brunswick. Can J Surg 56 (2 Supp) S28-S29.
Watson I., Hogan A., Woodford A., Benjamin S., Chisholm A., Ondiveeran H., Martin M. (2013) Impact of Rural Trauma Team Development Course (RTTDC) on trauma transfer intervals in a provincial, inclusive trauma system. Can J Surg 56 (2 Supp) S29.
Howlett M., Atkinson P., Doody K., Fraser J., Leblanc-Douchin D., Strack B. (2013) Trauma and stress: A critical dynamics study of burnout in trauma centre healthcare professionals. Can J Surg 56 (2 Supp) S29.
Atkinson P., Naveed A., vanRensburg L., Madan R. (2013) Ultrasound-guided pediatric forearm fracture reduction in the emergency department. Can J Surg 56 (2 Supp) S29.
Chesters A., Atkinson P. (2013) Block first, opiates later? The use of fascia iliaca black for patients with hip fractures in the emergency department: A systematic review. Can J Surg 56 (2 Supp) S29-S30.
Atkinson P., Fraser J., Verheul G., Parks A., Milne J. (2013) Simulation in trauma ultrasound training. Can J Surg 56 (2 Supp) S30.
Fraser J., Atkinson P., Benjamin S., Sproul E., Mehta A. (2013) Wake up: Head injury management around the clock. Can J Surg 56 (2 Supp) S31.
2012
Musgrave E. (2012) Trauma NB : A model of inclusivity. Outlook 35(1); 23-24.
Benjamin S., Hogan A. (2012) Closing the quality improvement loop: A collaborative approach. Can J Surg 55 Supp, S23.
Hogan A., Benjamin S. (2012) National Trauma Registry: “Collecting” it all in New Brunswick. Can J Surg 55 Supp, S23.
Fraser J., Atkinson P., Benjamin S. (2012) Does delay to initial shoulder reduction attempt affect success rate for anterior shoulder dislocation (pilot study)? Can J Surg 55 Supp, S23.
Martin M., Watson I, Hogan A., Benjamin S., Woodford S. (2012) Use of multidisciplinary, multi-site morbidity and mortality rounds in a provincial trauma system. Can J Surg 55 Supp, S23 –S24.
Recherche collaborative
Cliquez ci-dessous pour accéder aux travaux de recherche publiés en collaboration avec les membres de Trauma NB :
2025 Affiche de la conférence TAC
2024 Affiche de la réunion d’automne de la British Geriatrics Society
2024 Affiche du symposium sur la recherche en santé au Nouveau-Brunswick
2024 Affiche du symposium sur la recherche en santé au Nouveau-Brunswick
2024 La Conférence sur le Vieillissement du Réseau de Santé Horizon
2024 Affiche du symposium sur la recherche en santé au Nouveau-Brunswick
2024 Affiche de la conférence TAC
2024 Affiche du symposium sur la recherche en santé au Nouveau-Brunswick
2023 Réunion scientifique annuelle de la GSA

2023 Affiche de la conférence TAC